RESUMO
INTRODUÇAO: O objetivo foi avaliar a qualidade de vida e do sono da equipe multidisciplinar da Unidade de Tratamento de Queimaduras.
MÉTODOS: O questionário Short Form-36 Medical Outcomes Survey (SF-36) e o Pittsburgh Sleep Quality Index (PSQI) foram utilizados em 50 trabalhadores da unidade.
RESULTADOS: A limitaçao dos aspectos físicos, da saúde geral, da vitalidade e da limitaçao da saúde social e mental foram significativamente correlacionada com o sono (p<0,05).
CONCLUSOES: Esse ambiente de trabalho nao é propício para o autocuidado dos trabalhadores; ao contrário, é um lugar de mobilizaçao para emoçoes e para o estresse.
Palavras-chave:
Sono. Equipe de Assistência ao Paciente. Saúde do Trabalhador. Questionários. Unidades de Queimados.
ABSTRACT
BACKGROUND: The aim of this study was to assess the quality of life and sleep of the multidisciplinary team of the Burn Unit.
METHODS: The Short Form-36 Medical Outcomes Survey (SF-36) and Pittsburgh Sleep Quality Index (PSQI) were used in 50 workers.
RESULTS: The limitation of the physical aspects, the general health, vitality, and limitation of social and mental health were significantly correlated with sleep (p<0.05).
CONCLUSIONS: The work environment is not conducive to workers' self-care; rather, it is a mobilizing place for emotions and stress.
Keywords:
Sleep. Interdisciplinary Health Team. Workers Health. Questionnaires. Burn Units.
INTRODUCTIONThe burn is considered a tragedy in the lives of the patients and their families, meaning for health professionals one of the biggest challenges of hospital care
1. The pain of the burn is terrible for those who feel it and stressful for caregivers
2. During treatment, workers experience the challenge of caring, face harsh environments, generally warmer, to perform their work which result in uncomfortable conditions for multidisciplinary teams
3. Furthermore, they assist in alleviating the client's pain and sorrow, learning to live with intense sadness, trauma, discomfort, confused feelings, irritability, tension, anger, depression, abstinence syndrome, aggressiveness, stress, physical and psychological exhaustion
2. In multidisciplinary teams, inter-professional relations or interlinks with coworkers and with patients should be considered in order to understand the health aspect on the behavior of the patients professionals in relation to the workplace and social life.
The Burn Unit of Plastic Surgery Division provides patient care 24 hours a day, every day of the week, without administrative withdrawal. Employees are divided into shifts, so that services can be provided day and night unabated. In this context, the need to apply questionnaires that address various aspects essential to health, such as quality of life and sleep was observed.
This relatively unexplored subject does not have a great amount of scientific evidence able to respond to questions pertaining to Occupational Health in the hospital environment. The literature presented studies assessing quality of life and sleep, particularly in specific groups of health professionals such as nurses and doctors. However, an analysis of two aspects, through the applicability of the questionnaires Short Form-36 (SF-36)
4 and Pittsburgh Sleep Quality Index (PSQI)
5 individually, with a multidisciplinary team in the context of collective work was not found.
One reason for the increase of research on the topic of professional workers' quality of life and sleep is due to the negative impact of morbidity resulting from lifestyle and inadequate occupational conditions that affect the welfare of employees in the functioning and effectiveness of organization
6.
The aim of this study was to assess quality of life and sleep in the multidisciplinary team of the Burn Unit.
METHODS
Study designThis is an individual, observational, cross-sectional and analytical study.
PlaceThis study was performed at the Burn Unit of Plastic Surgery Division, Department of Surgery of EPM/UNIFESP.
SampleA sample of 50 workers (doctors, nursing staff - including nurses, nursing assistants, nursing technicians - and others) was selected to comprise the multidisciplinary team of the Burn Unit in this study. The subjects were selected according to the following inclusion and exclusion criteria.
Inclusion criteriaAge between 20 and 65 years, work at the Burn Treatment Unit, Regular exercise of profession and Graduate trainees in Medicine, Nursing and Physiotherapy.
Exclusion criteriaUnder 20 and over 65 years, healthcare workers apart from the Burn Unit, employees removed from position or function and workers from provisional services to the Burn Unit.
Study questionDo the professional category or day and night shift interfere with the quality of life and specifically to the quality of sleep in a multidisciplinary team in a Burn Unit at a tertiary Hospital?
Instruments (Questionnaires and domains)The Medial Outcomes Study-Item Short Form Health Survey (SF-36) consists of 11 questions and 36 items covering eight components (domains or dimensions), represented by physical functioning (ten items), social functioning (two items), role limitations due to physical problems (four items), role limitations due to emotional problems (three items), mental health (five items), vitality (four items), pain (two items) and general health perception (five items). The individual receives a score in each domain, ranging from zero to 100, zero meaning the worst score and 100 the best
7.
The Sleep Quality Index (PSQI) consists of seven components: the first refers to the subjective quality of sleep (i.e. the individual perception about the quality of sleep); the second to the sleep latency; the third to the sleep duration, obtained by the relationship between numbers of hours of sleep and the number of hours spent in bed but not necessarily asleep; the fourth to the habitual sleep efficiency; the fifth to the sleep disorders or conditions that compromise sleeping; the sixth to the use of medication, that is, whether or not the subject used sleep medications; and the seventh to the disturbances and daytime sleepiness, referring to the change in the willingness and enthusiasm to carry out routine activities. The maximum score is 21. Scores higher than five points indicate a poor quality of sleep pattern. The overall score is the sum of the seven components, each one ranging between zero and three points
8.
Validity of the questionnairesThe generic SF-36 is validated for the Brazilian population
4 as a tool for assessing the quality of life. The PSQI is validated for the Portuguese language as a specific instrument to measure quality of sleep
5.
Subject's ConsentAll subjects signed a Written Informed Consent after being instructed about the research, as approved by the Research Ethics Committee, under the protocol number 1611/10, respecting the Guidelines and Standards for Human Research.
Data CollectingData collecting covered the one-month period of November 16, 2010 - December 15, 2010. There were 50 respondents, all of whom met the selection criteria of the study. The aim of the study was explained to each participant by the researchers and then a written approval was required. The interview was performed individually in a private room at the Burn Treatment Unit, lasting about 20-30 minutes. Personal data was collected via an identification form. Each subject was instructed to read and answer questions honestly. Once done, the answers were delivered to the researcher.
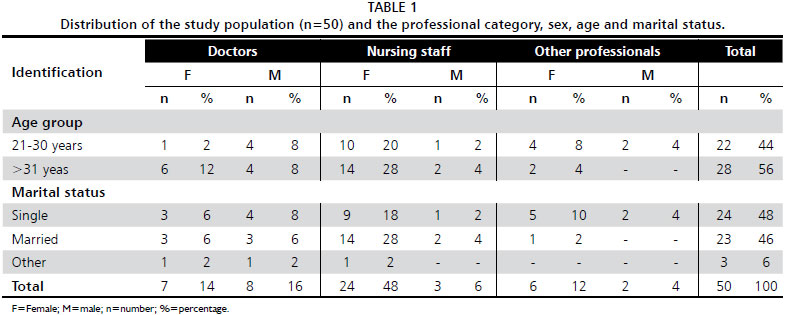
Twenty-seven were classified in the nursing staff category (27 - 54%), and 24 (48%) were female. Twenty-eight (56%) were older than 31 years and 24 (48%) were single (Table 1).
Statistical AnalysisThe following statistical analyses were performed. Kruskal-Wallis' variance test to compare the results of the eight domains of the SF-36 and PSQI sleep quality among the medical group, nursing staff and other professionals. Spearman's correlation was performed between sleep and each domain of the SF-36. Mann-Whitney test to assess the eight domains of the SF-36 and PSQI sleep quality between independent samples from day and night shifts was also used. For this, different professionals answered questionnaires if they work at day shift or at night shift, not the same person worked at day and night shifts. Friedman's analysis of variance was made among the eight domains of the SF-36 for each professional category and for day and night shifts. The rejection of the null hypothesis level was fixed at 0.05 (5%).
RESULTSFifty employees of the multidisciplinary team of Burn Unit were interviewed, distributed among doctors, nursing staff (including nurses, nursing assistants, nursing technicians) and others.
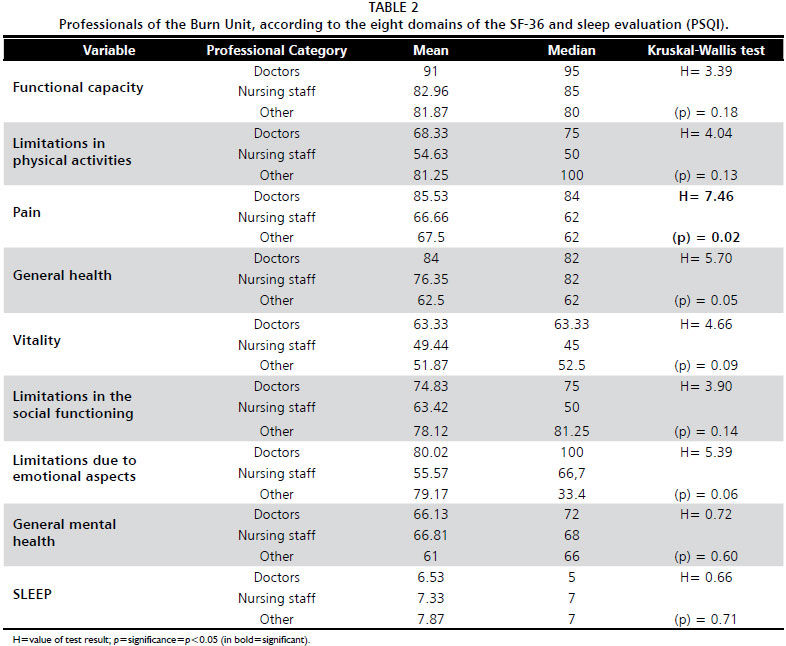
The Kruskal-Wallis' (Siegel's) analysis of variance was used to compare data of the eight domains of SF-36 and sleep between groups Doctors (15), nursing staff (27) and other professionals (8). Among the variables investigated, the pain domain of SF-36 had significant results for the different categories, showing that doctors have better quality of life regarding the pain (
p<0.05), as shown in Table 2.
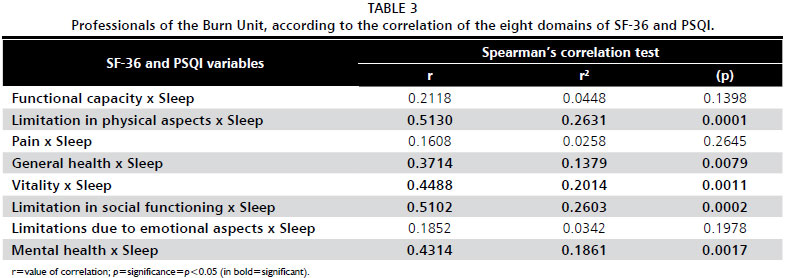
Spearman's correlation between sleep and each domain of the SF-36 revealed that the limitation of the physical aspects, general health, vitality, limitation of social and mental health were significantly correlated with sleep (
p<0.05). The limitation of the physical aspects obtained
p<0.0001 (Table 3).
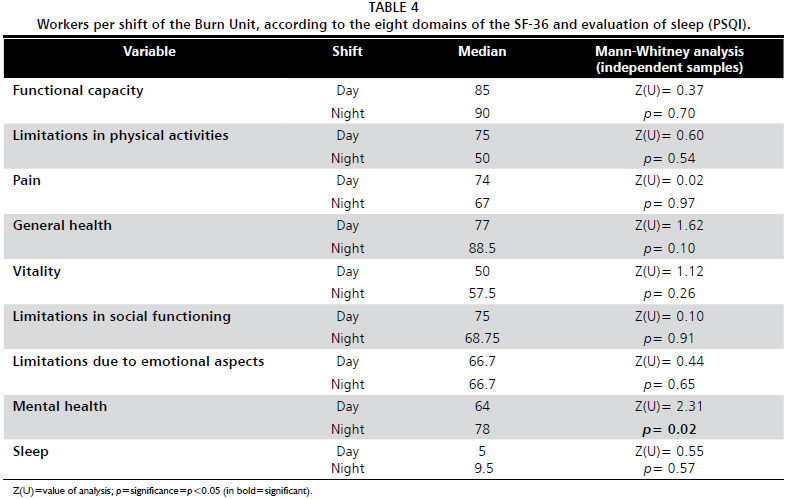
The Mann-Whitney test was performed to assess the data from the eight domains of SF-36 and sleep, between independent samples of day shift (31) and night shift (12), of which on-duty workers (7) were removed. In Table 4, it is possible to notice that mental health reported significant results (
p=0.02) when presenting night shift workers with better quality of life than the day shift workers.
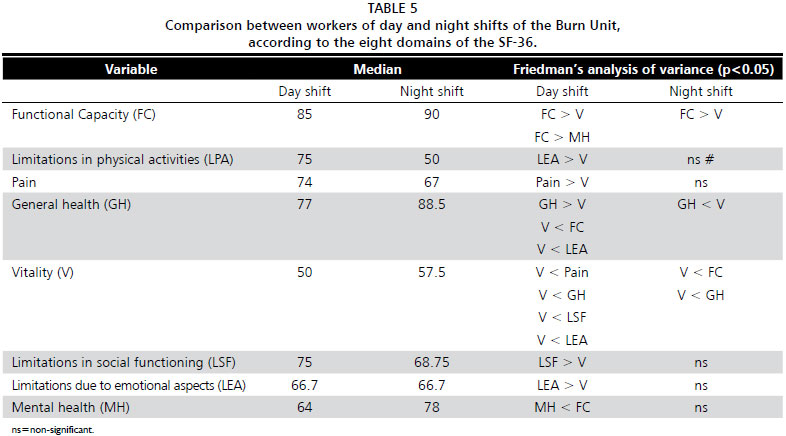
Regarding shifts, the Friedman's test found that, in day shift, vitality achieved significantly worse results than the domains of functional capacity, limitations in physical activities, pain, general health, limitations in social and emotional aspects; mental health showed significantly worse than functional capacity. In the night shift, vitality had worse results than functional capacity and general health (Table 5).
DISCUSSIONIn this study, the SF-36 and PSQI were applied in 50 individuals, of which females were prevalent (38 - 74%), a percentage slightly lower than the 89.9% reported in a similar study with a single professional category
9. These data reaffirm that, historically, the activities of caring for the sick, with its technological characteristics of watching, sanitizing, feeding, following the standards of social division of labor, have been and still are delegated to the female figure
10. The large contingent of female employees of the Burn Treatment Unit attracts attention as well as in other institutions, since the demand for physical effort in this unit is excessive and includes the preparation of shower and large wound dressings for burn-debilitated patients and the consequences of the treatment, escharotomies, debridement and grafts, which require immobilization or reduced mobility. Moreover, the high expenditure of muscular strength and excessive use of physical energy have caused problems in posture and general fatigue, becoming more severe as one finds a predominance of women in the labor force employed at the hospital
11.
Age ranged from 21 to 61 years with a mean of 33 years, with the majority (28 - 56%) older than 30 years, confirming studies in which 72.70% ranged from 20 to 40 years
10; 47.10% from 21 to 40 years
12; 76.20% from 35 to 49
13; 41.6% from 31 to 40
14; and 50% from 26 to 35
15. Although the mean age of the participants have pointed to a group of younger adults, one aspect observed among workers that could have health effects was the presence of professionals with age around 60 years
11. At this age there are some changes in the quality of life and health of the general population, such as higher chances of developing diabetes, hypertension, and/or obesity; being overweight; and going through menopause for women (who represents the majority of this study population).
Regarding marital status, twenty-four (48%) were classified as single and 23 (46%) as married. This last result does not differ much from the data of other authors
12,16, in which, respectively, 41.20% and 47.98% of the subjects were married.
In the professional category, it was observed that, regarding the pain, doctors had better quality of life than the nursing staff and other professionals (
p=0.02). General health, although not significant results in the analysis of variance of Kruskal-Wallis (
p=0.05), showed that doctors also have a better quality of life in relation to the others. These data corroborates another study
17 which pointed out that many professionals in the medical category are concerned about carrying out pleasurable activities, establishing priorities and avoiding excessive tension in their daily routine.
In the medical category, vitality had the poorest results compared to the domains of physical functioning, bodily pain, general health and limitations due to emotional aspects
18. Mental health presented worse results than functional capacity and general health. Similar results were reported by experts
10,19, who assessed the quality of life of residents of the operating room using the SF-36 and found impairment in emotional, social and physical vitality and mental health.
Regarding the nursing staff, it was noted that vitality achieved significantly worse results than functional capacity and general health; functional capacity showed better results than physical limitation. Among other professionals, vitality was significantly worse than limitation of functional capacity and limitations in physical aspects. The difference between the professional categories was justified in another study by interpersonal relationships in health team are referred by many professionals as a contributing factor to stress coming from the environment where they develop work activities
20.
Every nurse who is involved with the care of burn victims knows that stress is a part of burn nursing. Most of the time it is taken for granted that the various visual and psychological stressors are a part of our units. From the tragic accident to the elderly person or the curious child, the self-inflicted bum, the assault cases, the injustice of the abused or neglected child, the disabling or disfiguring burns, and the accidents that could have, or should have, been prevented - what an impact this must have on all of us. We practice a depth of teaching, we are witness to an amount of suffering, and we experience a level of involvement with our patients and their families that might be unique to burn nursing
21.
This study suggested that most of the stress reported by the burn nurses contains an emotional component, with issues relating to factors as follows: pain, the children, the dying patient, the patients who do not try to help in their recovery (perceived as uncooperative, manipulative, and/or angry), and interstaff conflicts, either nursing or medical. The most common methods of coping with work-related stress at work were talking with co-workers and maintaining a sense of humour. After work, the most common methods of coping came in the form of physical activity and talking with family and/or friends
21.
A burn unit that functions as a team and has a sense of team support most probably enhances the staff's ability to cope with the various stressors of their unit. Creating an atmosphere conducive for emotional venting and problem solving, and the involvement of supportive services such as psychology or chaplaincy may be beneficial in helping the nurses cope. Other areas of stress may be contended with increasing scheduling options, providing a means for further burn education, and keeping the patient to nurse ratio low. A recommendation would be that each unit should assess what are their areas of greatest stress for their nurses, how are the nurses coping with these stressors and what the unit itself can do to lessen the stress and promote coping. If the unit can develop methods for stress reduction in the workplace, the result may be increased coping and satisfaction for their nurses with the building of invaluable burn nurse experience
21,22.
The correlation between sleep and the domains of SF-36 had significant results (
p<0.05), in relation to limitation of physical aspects, general health, vitality, limitation of social aspects and mental health. These variables interfered with the quality of sleep of the multidisciplinary team, the reverse may also be considered in the correlation of these variables. This assessment suggests that a very demanding job can affect the quality of sleep, showing that the inference of work per shift may be milder than the type of work performed associated with quality of life of the individual. Regarding only the quality of sleep, twenty-six (52%) of the employees had poor quality of sleep, an estimate scarcely found in literature. A distinct instrument of PSQI found that 51.85% of the professionals had much altered sleep
23. It is noteworthy that, compared to other specialists
24 who found 92% of professionals with scores higher than 5, the multidisciplinary team at the Burn Treatment Unit has a good quality of sleep.
Between shifts, mental health was significantly impaired in the day shift in relation to the night shift, different result from the majority of published studies, in which night work is associated with essentially different a routine from the one adopted by the wider community in relation to the social and biological rhythms. The consequences for this type of employee include insomnia, irritability, drowsiness during the day, "hangover" feeling, chronic fatigue complaints, digestive malfunction, which in long-term lead to diseases related to gastrointestinal and nervous system and effects on work safety and quality of life of this group's member and their families
25,26.
Regarding the day shift, it was found that vitality achieved significantly worse results than the domains of functional capacity, limitation of physical aspects, bodily pain, general health, limitations in social and emotional aspects. It was noted that mental health presented worse results than functional capacity. In the night shift, vitality had the poorest results compared to functional capacity and general health. In the health area, schemes of work are different for each person, and night shifts are usually less frequent than the day shifts. Overnight activities are distinct from those determined for the other expedients
27. Shift work is a necessary and common practice in many organizations, especially in hospitals. It is a type of work schedule that considerably affects health professionals. Studies show that the interference in the personal relationship/family most often cited is the effect of shift work, followed by withdrawal of social activities and difficulty of life planning, living with the family, having friends and maintaining good social relationships
14,24.
The most affected domain among the professional categories and shifts was vitality, followed by physical aspects, emotional aspects, and mental health; similar results were found in a study in which most affected domains were pain, vitality, physical and emotional aspects
14. The lack of rest and entertainment triggers stress, which is considered a negative problem, of perceptual nature, resulting from the inability to deal with the work pressure sources. Stress is considered an important factor in pathological aspects of mental health and causes consequences mainly in the form of problems in physical and mental health; job satisfaction, which compromises workers' peer relationships due to the institutional demand; the organization of work and the lack of time for self-issues and self-care. Finally, the predominance of suggestions about interpersonal relationships and work organization bring the focus back to the individual, now as a professional in relationships within an organizational context with its peculiar characteristics. These characteristics do not prevent organizational transformation and restructuring, because the purpose is to ensure that the organization reaches both individual and organizational goals
10,25.
In multidisciplinary teams, inter-professional relations or interlinks with coworkers and with patients should be considered in order to understand the health aspect of the professionals' behavior in relation to the workplace and social life. This aspect is not the aim of this study, but it is important to be assessed, and some questions appear here, as what is the reason why some professional choose treat burns where they find difficult patients, most with psychic problems that there were before or that appear during the treatment. What kind of personality and psychological traits that lead professionals to work in a very difficult area, where tension is always present and suffering is the rule? This is an important question to be assessed.
There were some study limitations, like the literature found on the quality of sleep and quality of life of the workers is not abundant, meaning that it is not an ideal base to analyze the multidisciplinary team in a tertiary health care unit, or compare it to these results. The physical and mental mood, coupled with the daily events in the moment of the interview, could influence the data collection. Misinterpreted reading of the questions from SF-36 and PSQI may have occurred although the principal investigator and the supervisor were present during the interview to clarify questions contained in the surveys.
The workplace comprises repetitive routines, situations of risk, death and dying processes, and even suffering and pain of others. These experiences coupled with the bustle of everyday life lead individuals to seek defense or coping mechanism to handle stressors to which they are exposed. The mechanisms translate into disinterest in others, mechanical actions, failure to perceive the other as a human being, devaluation of care and self-devaluation as a person and professional. Therefore, the way work environments are currently structured does not favor employees' self-care; by contrast, they are naturally mobilizing places of emotions, feelings and stress
23.
The lack of rest and entertainment, justified by the most affected domains (vitality, physical, emotional and mental health) can trigger the devaluation of self-care, which hinders the ability to handle events in general. It is concluded that the structure of the current working environment does not favor such care, but rather mobilizes emotions, feelings and stress.
ACKNOWLEDGEMENTSWe would like to thank Leslie Fletcher for revising and commenting on this article. And thanks to the National Council for Scientific and Technological Development (CNPq), the Brazilian institution for funding scientific research by the scholarship. We would like to thank also all professionals working in the Burn Unit.
CONFLICT OF INTERESTAll authors declare that there are any financial and personal relationships with other people or organizations that could inappropriately influence this study.
REFERENCES1. Declair V. Atualizaçao em enfermagem em dermatologia. Rev Enferm Atual. 2003;17(4):36-7.
2. Rossi LA, Camargo C, Santos CMNM, Barruffin RCP, Carvalho EC. A dor da queimadura: terrível para quem sente, estressante para quem cuida. Rev Latino-Am Enfermagem. 2000;8(3):18-26.
3. Lacerda LA, Couto A, Oliveira AF, Gragnani A, Ferreira LM. Estudo epidemiológico da Unidade de Tratamento de Queimaduras da Universidade Federal de Sao Paulo. Rev Bras Queimaduras. 2010;9(3):82-8.
4. Ciconelli RM, Ferraz MB, Santos WS, Meinao IM, Quaresma MR. Traduçao para a língua portuguesa e validaçao do questionário genérico de avaliaçao de qualidade de vida SF-36 (Brasil SF-36). Rev Bras Reumatol. 1999;39(3):143-50.
5. Bertolazi AN, Fagondes SC, Hoff LS, Dartora EG, Miozzo IC, de Barba ME, et al. Validation of the Brazilian Portuguese version of the Pittsburgh Sleep Quality Index. Sleep Med. 2011;12(1):70-5.
6. Magalhais LCB, Yassaka MCB, Soler ZASG. Indicadores da qualidade de vida no trabalho entre docentes de curso de graduaçao em enfermagem. Arq Ciênc Saúde. 2008;15(3):117-24.
7. Ware JE Jr. SF-36 health survey update. Spine (Phila Pa 1976). 2000;25(24):3130-9.
8. Buysse DJ, Reynolds CF 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193-213.
9. Aguiar ADF, Barreto EO, Aguiar KS, Biazzini MG, Silva PM. Saúde do trabalhador de enfermagem que atua em centro de saúde. Rev Inst Ciênc Saúde. 2009;27(2):103-8.
10. Oler FG, Jesus AF, Barboza DB, Domingos NAM. Qualidade de vida da equipe de enfermagem do Centro Cirúrgico. Arq Ciênc Saúde. 2005;12(2):102-10.
11. Schmidt DRC, Dantas RAS. Qualidade de vida no trabalho de profissionais de enfermagem, atuantes em unidades do bloco cirúrgico, sob a ótica da satisfaçao. Rev Latino-Am Enfermagem. 2006;14(1):54-60.
12. Rezende MP, Robazzi MLCC, Secco IAO, Suazo SVV. Riscos físicos e sua identificaçao por auxiliares de enfermagem de hospital de ensino do estado de Minas Gerais, Brasil. Rev Enferm UFPE On Line. 2009;3(3):152-9.
13. Talhaferro B, Barbosa DB, Domingos NAM. Qualidade de vida da equipe de enfermagem da central de materiais e esterilizaçao. Rev Ciênc Méd. 2006;15(6):495-506.
14. Pereira MCA, Favero N. A motivaçao no trabalho da equipe de enfermagem. Rev Latino-Am Enfermagem. 2001;9(4):7-12.
15. Aldrighi JM, Alecrin IN, Oliveira PR, Shinomata HO. Tabagismo e antecipaçao da idade da menopausa. Rev Assoc Med Bras. 2005;51(1):51-3.
16. Costa ES, Morita I, Martinez MAR. Percepçao dos efeitos do trabalho em turnos sobre a saúde e a vida social em funcionários da enfermagem em um hospital universitário do estado de Sao Paulo. Cad Saúde Pública. 2000;16(2):553-5.
17. Gasperi P, Radunz V. Cuidar de si: essencial para enfermeiros. Reme Rev Min Enferm. 2006;10(1):82-7.
18. Santos TCMM, Inocente NJ. Ritmicidade biológica e qualidade de sono em enfermeiros [Internet]. In: X Encontro Latino Americano de Iniciaçao Científica e VI Encontro Latino Americano de Pós-Graduaçao da Universidade do Vale do Paraíba; Taubaté [citado 2007 Nov 18]. Disponível em:
http://www.inicepg.univap.br/trabalhos/EPG00187_04C.doc .
19. Franco GP, Barros ALBL, Nogueira-Martins LA. Qualidade de vida e sintomas depressivos em residentes de enfermagem. Rev Lat Am Enferm. 2005;13(2):139-44.
20. Silva JLL, Melo ECP. Estresse e implicaçoes para o trabalhador de Enfermagem. Inform Promoç Saúde. 2006;2(2):16-8.
21. Lewis KF, Poppe S, Twomey J, Peltier G. Survey of perceived stressors and coping strategies among burn unit nurses. Burns. 1990;16(2):109-12.
22. Medeiros SM, Ribeiro LM, Fernandes SMBA, Veras VSD. Condiçoes de trabalho e enfermagem: a transversalidade do sofrimento no cotidiano. Rev Eletrônica Enferm. 2006;8(2):233-40.
23. Barboza JIRA, Moraes EL, Pereira EA, Reimao RNAA. Avaliaçao do padrao de sono dos profissionais de Enfermagem dos plantoes noturnos em Unidades de Terapia Intensiva. Einstein. 2008;6(3):296-301.
24. Lentz RA, Costenaro RGS, Gonçalves LHT, Nassar SM. O profissional de enfermagem e a qualidade de vida: uma abordagem fundamentada nas dimensoes propostas por Flanagan. Rev Latino Am Enfermagem. 2000;8(4):7-14.
25. Rotenberg L, Portela LF, Marcondes WB, Moreno C, Nascimento CP. Gênero e trabalho noturno: sono, cotidiano e vivências de quem troca a noite pelo dia. Cad Saúde Publica. 2001;17(3):639-49.
26. Oliniski SR, Lacerda MR. Cuidando do cuidador no ambiente de trabalho: uma proposta de açao. Rev Bras Enferm. 2006;59(1):100-4.
27. Gadbois CH. L'exacte mesure des situations de travail posté: au-dela des similitudes formelles, des réalités différentes. Trav Hum. 1990;53(4):329-45.
1. Graduate Student, Federal University of Sao Paulo/Paulista Medical School, Sao Paulo, Brazil
2. Associate Professor of Plastic Surgery Division, Federal University of Sao Paulo/Paulista Medical School, Sao Paulo, Brazil
3. Graduate Student, Federal University of Sao Paulo/Paulista Medical School, Sao Paulo, Brazil
4. Nurse-in-Chief of the Burn Treatment Unit of Hospital Sao Paulo, Sao Paulo, Brazil
5. Full Professor of Public Health Division, Medical School of University of Santo Amaro, Sao Paulo, Brazil
6. Chairwoman, Full Professor of the Plastic Surgery Division, Federal University of Sao Paulo/Paulista Medical School, Sao Paulo, Brazil. Burn Treatment Unit of Plastic Surgery Division
Correspondence:
Alfredo Gragnani
Division of Plastic Surgery of the Federal University of Sao Paulo/Paulista Medical School
Rua Napoleao de Barros, 737 -4º andar. Vila Clementino
Sao Paulo, SP, Brasil - CEP 04024-002
E-mail:
alfredogf@ig.com.brThe authors disclose any commercial interest that they may have in the subject of study and the source of any financial or material support.
This study was carried out at Federal University of Sao Paulo/Paulista Medical School, Sao Paulo, Brazil.


 Português PDF
Português PDF Imprimir
Imprimir
 Enviar este artigo por email
Enviar este artigo por email
 Como citar este artigo
Como citar este artigo
 Enviar um comentário
Enviar um comentário
 Mendeley
Mendeley
 Pocket
Pocket
